You are here
Faculty test-beds - Gloustershire: a model
Dr Jane Melton MBE FRCOT PhD is Interim Lead for Allied Health Professionals, One Gloucestershire ICS and Interim Regional Chief AHP, South West NHS E/I.
The Opportunity
The One Gloucestershire Integrated Care System set up their AHP Council in March 2019. It has 35 members, is an expert advisory group and a connecting forum to the whole health and care system. Through Jane's leadership, the AHP Council members and the ICS leaders saw the HEE funding as an opportunity to secure a decision-making forum of very senior AHP leadership. They formed a faculty, seized the leadership opportunity and now report into the wider AHP Council. The faculty has afforded them set time across agencies, to really deep dive into what they needed to do to enhance their AHP workforce across lots of domains. They applied to take a rounded approach to the faculty and workforce, which was less about the money and more about the validation of their idea.
The Gloucestershire faculty used the HEE funding to create leadership capacity to drive this work; formal project management and events/conferences to bring the system together and co-produce solutions. "Having a faculty has helped our AHP Council mission by enhancing our influence and voice. Immediately in our system, there was a common goal for AHPs to complement the perspectives of our traditionally medically orientated leadership".
Chairing
As chair, Jane pulled together Chief AHP leads to have a weekly meeting focused on solutions to enhance clinical placement capacity: “These started as 30-minute conference calls and we were fortunate that this routine got us to a good place which took us through to COVID-19. We then repurposed the meetings to think about what we needed to do as a system to respond to the pandemic - for example workforce and clinical placements.”
Bringing together the right blend of organisations, people and skills are crucial. As an effective leader in a position of chair, a proactive approach to understanding the dynamics of the system and continue supporting your members is essential. It is a credit to Gloucestershire's Integrated Care System that the capacity has been created for this.
Membership
Selecting AHP Faculty members was straightforward. Gloucestershire ICS has a neat structure and serves a population of approximately 700,000 people across the provider landscape. There is only one acute NHS provider and the solo community provider also hosts an AHP social care contract. AHP Faculty members represent each of the following organisations.
- Gloucestershire Health and Care NHS Foundation Trust (community, mental health and learning disabilities services)
- Gloucestershire Hospitals NHS Foundation Trust (acute hospital services)
- NHS Gloucestershire Clinical Commissioning Group
- SW Ambulance Service NHS Trust
- Gloucestershire County Council
- Primary Care Services
- University of Gloucestershire
- Cobalt Health (independent sector)
The chief AHP for the community trust and the chief AHP from the acute trust are members (N.B. neither are called that but are the most senior AHPs in their organisations). They both report to their respective Directors of Nursing which is a crucial reporting line and source of support.
Senior social care colleagues sometimes attend and we are working together to ensure social care perspectives are included in developments. Having the membership of the Head of School from the local university is also key as they connect into many relevant work streams at the university.
Membership also includes the Research Lead from a local imaging charity who bring a fresh perspective, rapid decision making and can-do approach. The local ambulance service are members but also cover a wider geographical area. They are very active and because of their wider south-west of England remit, they can’t always attend meetings. Instead, Jane liaises with them separately to ensure that they are connected into the work and able to influence the way forward.
The faculty is currently considering the next potential wave of membership, including local private hospitals who have been very involved in the COVID-19 response with their AHP workforce.
Key skills
Senior leaders have varying levels of capacity, so it’s important to respect people’s availability and to lead with the behaviours that you want to engender. "I think it's important to put my own hand up and volunteer for tasks, drawing in colleagues who have limited time to review, challenge and contribute to the work that I lead. We are really lucky to have some people with unique skills in our faculty, for example, our primary care development lead brings something different from her experience that’s helping us move forward with the workforce in a new area".
Effective communications and sharing intelligence has become part of our business as usual in Gloucestershire’s AHP faculty. "We’re ensuring that AHP leaders are sharing messages about the effectiveness of our work and it's meaning for service users to make the most of our offer and to make a difference. Regular action points require faculty members to cascade messages back to their respective organisations to share and communicate, in fact one of our bid outcomes was to “Share our results locally and nationally.”
Governance
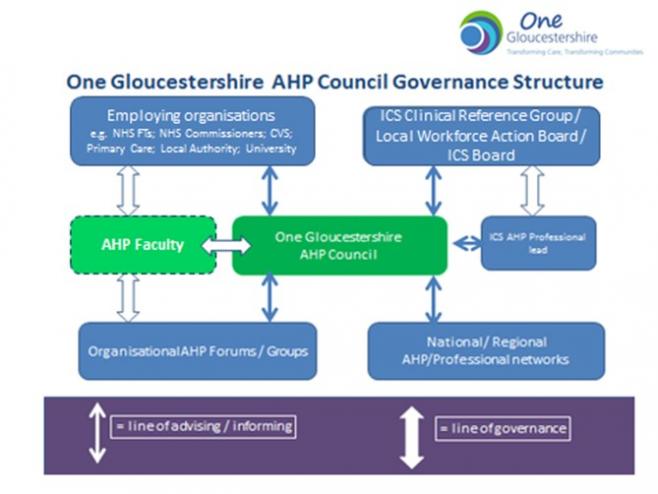
Governance helps us to assure what we are doing is effective, connected and has a positive impact in our system. We created a joined-up reporting structure to ensure our AHP faculty and AHP Council has visibility and engagement across a diverse range of decision-makers (see Figure 1 below).
- Jane reports into her manager in the CCG – the Director of Nursing
- Jane reports into the LWAB chaired by the CCG's Accountable Officer
- Jane reports into the CCG clinical forum to ensure the CCG's Medical Director is sighted
- Replicating this across all members is important – and especially linking in with the Directors of Nursing in the various organisations
- Encouraging the other faculty members to report back is part of fostering the continual loop of information sharing and improvement
- Jane is involved in the right approach for succession planning for the ICS AHP role and is working on a sustainability plan for the future
Levers of influence
Levers of influence are considered by Gloucestershire's AHP faculty members and how we use them to best effect. The head of school at the local HEI has a wide set of people to engage with and these are, in the main, different and complementary to our Chief AHPs. For example, AHP matters are drawn to the attention of the vice-chancellor of the University and research teams through the HEI and NHS Executive directors via our Chief AHPs. With private and third sector partners, Gloucestershire's AHP faculty are looking at how we best collaborate in the interests of the people we serve in order to do things differently, where traditionally, people may not have collaborated. It’s important to consider what influence people have, how we keep it all connected and crucially how they can work together effectively and not in opposition.
The use of data is a powerful lever of influence and can be uncovered and utilised in your system. The AHP Council recently sent a letter of thanks to AHPs across the county for their passion and commitment during the COVID-19 pandemic. The dissemination of the letter was very interesting as it required significant background work for the larger organisations to identify the names of all AHPs in their workforce. This is exactly the kind of opportunity an AHP Faculty can capitalise on to build and consolidate high-quality data that will be useful for other scenarios going forward.
Leadership and visibility
The faculty structure does not necessarily give authority to act, but it is a great opportunity to inspire energy for action as well as momentum for development and change. It takes courage to be visible, to challenge the norm, to bid, to publish and present. "It's important to remember that engaging with these things won't necessarily feel or be perfect from the start. Have a final vision in mind, embrace evolution, learning together and evaluate. That way, we are modelling leadership and giving people permission to behave as leaders and assume leadership in a whole systems approach".
"I’ve been very fortunate in my career. I have had the good fortune to believe that I can make a difference. I have sought out good people who could help me lead and achieve client-centred goals with a collaborative approach. Mentorship and coaching is important for aspiring leaders and I would certainly encourage people to seek such support. My background is Occupational Therapy. It is natural to me to use Occupational Therapy Theory[1] to guide me in my leadership. I reflect on:
- My sense of volition including my belief in my own ability, my interests and my obligations as a leader to motivate my actions
- My habits, for example my routines, roles and what I draw in and prioritise to support my leadership
- My own capacity for performing the various aspects of my role - health and wellbeing is important to be mindful of
All of these things dynamically interface with my environment. As a leader, I see myself as facilitating the environment to get a task done and to ensure sustainability. Leaders have to consider whether the opportunity which has presented will realise benefits towards the goals set.
Playing your part in developing a culture of meaningful, energetic, courageous leadership with ideally shared action is essential. This is why I like to lead through action. I’m content to put myself forward and ask others to inform and critique my work.
The AHP agenda is massive. There’s power and wellbeing in understanding you haven’t got to fix things all by yourself just because you have a leadership role. Coaching can have great impact in helping people to understand what the challenges have been along the way and crucially to help people see they have influence in lots of different spheres. AHP leaders wear so many different hats, so it’s important that they are able to join those dots and are aware of their potential to influence different but connected agendas.
The idea of developing a local AHP Faculty has certainly been worthy of our shared leadership effort.
RECIPE CARD
A key checklist to drive value and success in an AHP Faculty
- Governance and reporting structures: ensure you have visibility and accountability within each member’s respective governance, and collectively within STPs & ICS. Ensure there is two-way flow and feedback of reporting to nursing, medical and system chief officers
- Frequency of meetings: 30-60 minutes weekly allows for agility and momentum that is responsive to emerging needs and ensures a constant sharing of information
- Membership makeup: Think about the needs of your local health and care ecosystem. Support AHP leads and champion the introduction of AHP leads in commissioning and provider organisations. Don’t be afraid to look to other stakeholders in the private and voluntary sector if they can add drive and capacity to the objectives of the faculty. There is a responsibility for the chiefs to be sitting on it, and wider groups to achieve the richness of the developments that we wanted to achieve.
- Chairing: You must create capacity for an experienced chair to work in a flexible way with members. Lots of work will happen within the official meetings, but there’s a lot of liaison, communication and influencing that takes place outside of it too.
- Shared purpose and learning: make this your manifesto, co-produce it where you can, but also don’t be scared to step confidently into that leadership role yourself. Regularly check that members understand the shared purpose
- Continuous improvement: use the plan, do, study, act (PDSA) improvement model to develop, test and implement changes
- Leadership:
- nurturing leadership
- encouraging involvement
- sharing the responsibly for things where’s that warranted
- holding people to account (but being kind)
- collaborate and share the load – whilst bringing in project management support to do things like writing the plan and coordinating contributions
- build in flexibility to adjust the plan in order to be able to deliver
- look for opportunities and funding to provide leadership training for all faculty members to continue the shared leadership approach across their respective parts of the ecosystem
- Data: What datasets do you need and do you have a dashboard? Verify and triangulate datasets as you ascertain their reliability. Use data to understand your faculty’s means of and ability to problem solve; How successful you are in implementing solutions and prioritising them?
- Be Action orientated: the action log from faculty meetings can be a good indicator of energy, purpose and pace. Use this is a check for gauging culture and momentum
- Levers of influence: consider what levers of influence faculty members have and how they are using them. Dissemination of information, reporting up, cascading and gathering knowledge
[1] Taylor R.R (2018) Taylor R.(Ed) Kielhofner’s Model of Human Occupation (5th Ed). Wolters Kluwer