You are here
Case Study: Devon
Vicky Webb, Independent Prescribing Clinical Lead. University Hospitals Plymouth
What made you bid for the teach and treat funding?
- desire to engage in collaborative system-level working
- prioritise community pharmacists to get as many to achieve their Independent Prescriber (IP) qualification as possible and then see how we can transition them to DPS and DPP in time for September 2025
- establishing any model that expands supervision capacity ahead of next September was needed
- key stakeholders were mostly based in general practice as these are the relationships that must continue beyond the course and will lay the foundation for safe IP in community pharmacy
What were your outcomes?
Primary outcomes
- increase the number of independent prescribers in community pharmacy. Aiming for 20 in the first year of the pilot and 40 in the second year
- establish a sustainable model of supervision
Secondary outcomes
- setup a community of practice for community pharmacist independent prescribers
- facilitate relationships between the primary care networks and community pharmacy
- raise awareness of the role of the designated prescribing practitioner (DPP)
- increase DPP capacity, particularly in the context of IETP reform coming into force from 2026
What did you do?
I was recruited into a dedicated role to be the strategic lead for this pilot.
EOI process was already live, and 10 community pharmacists identified to start their prescribing with Teach & Treat (T&T) support from September.
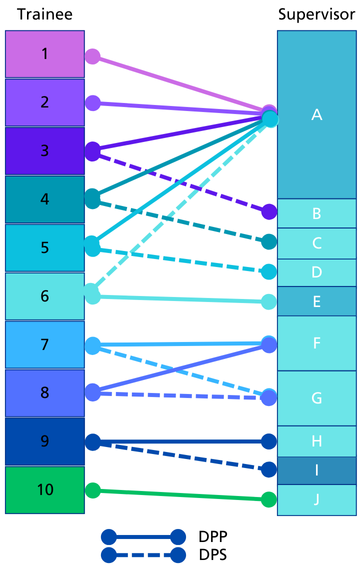
There was a vision for a hub and spoke model, with me as a hub coordinating supervision, and a spoke being DPP to multiple pharmacists.
Identifying supervision for the rest of the group meant asking as many people as possible until I had sufficient positive responses. Letters sent to every practice via Devon training hub, direct email comms to practices within trainee IP network, following up on any networking contacts, email to all IPs at UHP, a ton of networking and meetings. Common queries needed to be addressed- DPP role expectations, time required, funding available.
I’m supervisor A in figure 3, fulfilling 35% of the supervision capacity for the first September 2023 group.
Certainly, DPP myth-busting was top of the list. I produced a poster to send out and hosted a lunch and learn session via Devon training hub. I delivered a similar session via our ACP forum in the trust.
Being able to offer funds to host organisations has been invaluable to be honest.
Challenges/barriers from host organisations are nearly always that they have existing training commitments that prevent them from taking on anyone else from outside the organisation. Shortly followed by not enough money on offer to make it worth their while.

I’ve also done a lot just to raise the profile of the project with the hope of making future buy-in easier, presented a poster at regional pharmacist research conference and two local multi-professional research conferences. Session and poster at CPC London.
Published initial project report in PM journal in January. Working on the second article at present.
What happened?
- supervision identified for 11 pharmacists to start their course in September 2023. 1 deferred the start of the course. 1 withdrew at the midpoint. 6 have confirmed that they have passed the course. 2 have resubmits. 1 is unknown
- 2 started in January 2024 and have passed their assessments, just waiting on portfolio outcome
- supervision identified for 12 to start their prescribing in March 2024. Two missed out on March start as course oversubscribed. 1 apparently deferred the start of the course but didn’t notify me. Currently 9 in progress
- we’re on track to get 20 through their IP in the first academic year.
- now we’re preparing for the start of the September 2024 group we’re in a much stronger position as a lot of my previous DPPs and DPSs are hosting subsequent trainee prescribers. I haven’t analysed numbers yet
Sustainability
None of our IPs is able to use that qualification yet. They have reported that the quality of their consultation is significantly improved, and they feel this has had a really positive impact on their ability to deliver Pharmacy First. Improved documentation and improved referrals have also had initial impact on some on GP CP relationship, but this hasn’t been formally analysed.
There hasn’t been sufficient time passed for any of them to act as DPP or DPS. They also need to be in an environment where they are routinely prescribing.
Scalability
We are very much in need of the pathfinder sites to be consistently online and then perhaps a program to help rotate our newly qualified IPs through these sites. Particularly if they are employed by the same organisation.
Need to get supervision of CP trainee IPs integrated into normal workflows. All IETP providers hosting trainee pharmacists from September 2025 could host a community pharmacist trainee IP, alongside their final year trainees. They could experience the same 90 hours of supervised practice learning.
The main takeaway from our pilot is that a multi-professional, cross-sector model of supervision, can work. You can absolutely take a community pharmacist and place them with a nurse in a hospital to help them achieve their IP qualification.
Testimonies
All respondents identified a positive aspect of doing their supervised practice hours in a different clinical environment. There were three main themes identified.
Opportunity to work with and observe different members of a multidisciplinary team
“Better understanding of different roles and opportunities”.
“A wider variety of experiences, a bigger pool of experience to draw upon, more contact with already qualified IPs,”
“Able to see how other practitioners work in a different setting”?
Improved confidence and practice
“Different environment has improved my confidence and benefited by gaining some experience”.
Dedicated time to learn
“No distraction by day job”
When asked about disadvantages of completing supervised practice in a different area, only two respondents offered a specific answer. The main theme was that the learning in that environment is not always directly applicable.
“I felt like the hospital elements weren’t particularly useful for me as I was with a prescribing nurse and hospital is not an area I am interested in. This may have been different if I had considered hospital pharmacy though!”
“May not be applicable to my usual practice.”
Overall, all were satisfied with their experience of completing the supervised practice hours in a different environment to where they normally work (50% very satisfied, 50% somewhat satisfied).
When asked what could have made the experience better, these were the following suggestions?
“Being with a prescribing pharmacist”.
“More support from my Employer”
“From a personal point, the travelling time to sessions was challenging”.
“DPP and other participants were very helpful.”
DPP/DPS responses
All respondents reported being satisfied with their experience of supporting a community pharmacist trainee prescriber; 83.3% very satisfied, 16.7% somewhat satisfied. All respondents also stated they would supervise a trainee prescriber as part of the T&T project in the future.
Supervisors were asked if there was 'anything that would have made this experience better?' Two people offered responses
“As with most things, I expect the experience is very person specific. My first trainee through T&T fitted well with the team and was an absolute pleasure to teach and work with. I suspect my answer to this question may be very different depending on the student, but for the first experience of T&T, no more improvement is needed.”
“The trainees are superbly interested; they just don’t have the depth and breadth of knowledge to make decisions and will end up being an antibiotic dispensary. It won’t work without proper training, and that’s medical school.”
Reflections: Top Tips
I will definitely keep the teaching sessions. They’ve been received very well and there is a keen appetite for this small group learning environment to continue beyond the course.
How long did this process take? Could it have been delivered faster, and if so, how?
15 months in post and 20 through their prescribing so far. I don’t think I could have done this any faster.
What were the difficulties or challenges you faced and how did you overcome them?
Personally, undergoing significant CPD so that I could selectively expand my scope to better support my trainees. Identifying an ED consultant as my own clinical supervisor has been instrumental with this.
There have been challenges with HEIs- varying DPP/DPS requirements, varying assessment requirements for the trainees, different and changing cohort dates, different application timelines, delayed application opening and then early application closing, oversubscribed courses.
There have been significant challenges with getting stakeholders on board, but when DPPs/DPSs have been identified there haven’t been many issues. Only one DPP I had to replace because her email response times were so poor the trainee missed the application deadline.
Administratively, instructing purchase orders and ensuring all the correct information that procurement require is laborious to say the least. Similarly, arranging honorary contracts and OH clearance for each trainee for what might only be 45 hours 1:1 with me, seems excessive. Some of this seems to duplicate checks required by the university to do the course. And if they are registered professional employed by an organisation delivering NHS services, surely that should be sufficient. The required admin takes a significant chunk of my time.